Ricochet of a Lie
And Kennedy’s Throat Wound
(A version of this essay was previously published under the title “The Magic Throat.”)
If you believe the gaping hole in the front of Kennedy’s neck was the result of body alteration by unknown persons, the facts below may change your mind.
Commander James Humes, M.D., the lead pathologist who performed the autopsy on President John F. Kennedy, was interviewed in 1992 by the Journal of the American Medical Association (JAMA).1 Once again, he and his team were going to set the record straight.
As often happens on these occasions, Humes provided a fresh crop of contradictions. One such contradiction is the subject of this article: the size Humes gave JAMA for the incision in Kennedy’s throat: less than half the size he reported earlier,2 3 and less than half the size as it appears in autopsy photographs.
What intrigues me about this new size is its striking similarity to the one described by Malcolm Perry, M.D., to David Lifton, author of “Best Evidence.”4
1964, James Humes: Large Incision
According to Humes’s autopsy report,5 the tracheotomy incision was 6.5 centimeters, but Humes told the Warren Commission it was between 7 and 8 centimeters.6 The latter description seems to match what shows in autopsy photographs. (Note: “tracheotomy” is sometimes spelled “tracheostomy”; both are correct.)
1980, Malcolm Perry: Small Incision
The best selling Best Evidence by David Lifton was published in 1980. In it, Lifton quotes Malcolm Perry as saying the incision was only 2 to 3 centimeters wide. When Lifton asked if it could have been 3.5 centimeters, Perry agreed. Could it have been 4 centimeters? Perry “hesitated a bit, then said yes.” How about 4.5 centimeters? Perry said he “really doubted it was that large. It just wasn’t necessary.” Lifton added, “Perry sounded distinctly uneasy.” Lifton quoted other Parkland doctors who corroborated Perry’s claims.7
Perry’s first answer, “2 to 3 centimeters wide,” is consistent with the routine tracheotomy incision as diagrammed in Lifton’s book.
Not the kind of incision made on a victim of a penetrating neck trauma.
1992, James Humes: Small Incision
Humes told JAMA that “The tracheostomy was a gaping wound, about 3 to 4 centimeters around ….”8
Only 3 to 4 centimeters “around”? This is how one describes a perimeter. Translated, this would make the incision across no more than 2 centimeters in horizontal width—about the size Malcolm Perry gave David Lifton. A very interesting match indeed.
What Did Malcolm Perry Actually Do?
Small incisions are created for routine tracheotomies—the kind performed for patients with severe breathing problems, such as those due to pneumonia, for instance. David Lifton investigated and then publicized the appearance of a routine tracheotomy incision.
What David Lifton did not investigate at all, apparently, was this relevant question:
How do emergency room doctors respond to a penetrating wound in the neck, regardless of whether the patient has wounds elsewhere in the body?
Doctors must quickly find and repair any life-threatening damage that has been done—and that means creating a fairly wide incision, one large enough to visualize the carotid arteries, for example. (These arteries are not in the middle of the throat; they are off to either side of the neck.)
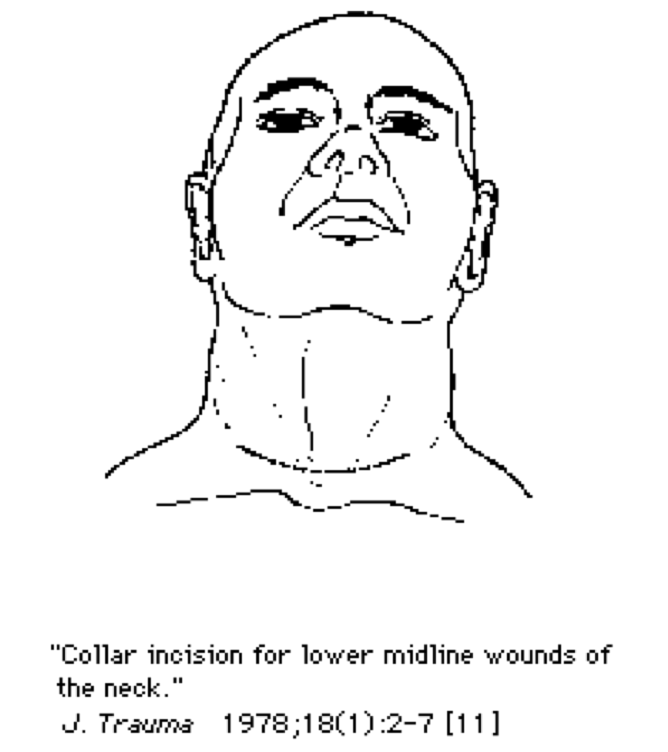
From Perry’s and Humes’s descriptions, it sounds like Kennedy had a “collar incision,” similar to the one shown below from the Journal of Trauma 1978; 18 (1) : 2-77 (see the Addendum at the end of this article for more extensive documentation).
In Kennedy’s case, it was already clear that he was having trouble breathing, and one doctor placed an endotracheal tube which proved to be inadequate. So when Perry arrived, he performed a tracheotomy. And, he said, he “made an incision right through this wound which was present in the neck.”9
But that was not all that Perry did. He made an incision large enough to allow him to inspect the carotid arteries, the mediastinum, and other structures.
“Once the transverse incision through the skin and subcutaneous tissues was made, it was necessary to separate the strap muscles covering the anterior muscles of the windpipe and thyroid. At that point, the trachea was noted to be deviated slightly to the left and I found it necessary to sever the exterior strap muscles on the other side to reach the trachea.”10 (His testimony on another day is similar.11)
“I also made it big enough that I could look to either side of the trachea … I didn’t know whether I was going to encounter carotid arteries or whatever. But the path of the bullet clearly put those vessels at risk as well as the trachea, so I made the wound big enough to do that … How big it [the incision] was, I don’t know … . I made it big enough to control an underlying bleeding blood vessel if necessary.”12
Please see the Addendum for quotations from articles on this subject—including some from a chapter in a textbook written by Malcolm Perry himself.
Why Perry Described Such a Small Incision: A Theory
Malcolm Perry was aware of Humes’s sworn testimony that, on the night of the autopsy, he knew nothing about a bullet wound in the throat, that he thought only a tracheotomy had been done.
Caught off guard by Lifton’s question, Perry probably thought he had better not say anything that would contradict Humes’s story.
Perry was apparently confident that Humes’s earlier report of a large incision was not well known. He has said more than once that he never met anyone who had read the Warren Commission Hearings.
Why Humes Revised the Size: A Theory
Small incisions are not done in the presence of a penetrating wound in the throat.
If Kennedy only had a small opening in his throat, this would have made it easier to believe Humes’s story of thinking the president only had a tracheotomy. This may have been the reason Humes gave such a different description of the incision to JAMA.
Furthermore, he may have worried that, had he described a wider incision, one that was more consistent with those performed in the presence of trauma, then one of JAMA’s readers might well have asked, how could he have been so sure the only abnormality in JFK’s throat was the remains of a tracheotomy? Especially in the presence of a bullet wound in the back?
What May Lie Behind the Revisions
Had Humes admitted to being aware of a throat trauma, he would have then been obliged to deal with it: dissect its path, obtain tissue specimens, document its characteristics, photograph it close-up and under magnification.
What if a proper study of the wound showed it to be an entrance? This would mean that at least one shooter was in front of Kennedy. But Humes and his team were under a great deal of pressure to prove the president’s wounds were created by one sniper, located above and behind.
Better to feign ignorance of a wound that may contradict that conclusion. Better to wait until after the body was gone, when it was too late to document its nature—entrance or exit—and its alleged connection with the wound in the back.13
But Humes Did Know
It seems that, even on the night of the autopsy, Humes et al. did know that a bullet had passed through Kennedy’s throat, either coming or going.
The bruising in the neck is what told him, bruising that could only have occurred during the motorcade—when the heart was still beating normally. What’s more, possibly out of vanity (and to avoid looking stupid to his peers), he wanted the Warren Commissioners to know that he knew, that he had not missed something so important, or its significance.
“When examining the wounds in the base of the President’s neck anteriorly … we noted, and we noted in our record, some contusion and bruising of the muscles of the neck of the Present. We noted that at the time of the postmortem examination.”14
He went on to describe wounds that were created by the Parkland doctors: incisions made in the chest for the placement of chest tubes, and in the arm and ankle for administering intravenous fluids—wounds that did not lead to bleeding and bruising, because they were made later, when the heart was barely beating.
“Those wounds [made at Parkland, on the chest and in the arm and ankle] showed no evidence of bruising or contusion … which made us reach the conclusion that they were performed during the agonal moments of the late President … when the circulation was … seriously embarrassed, if not nonfunctional. So that these wounds … were performed about the same time as the tracheotomy wound …”15
“So, therefore, we reached the conclusion that the damage to those muscles on the anterior neck just below this wound were received at approximately the same time that the wound here on the top of the pleural cavity was, while the President still lived and while his heart and lungs were operating in such a fashion to permit him to have a bruise in the vicinity … so we feel that, had this missile not made its path in that fashion, the wound made by Doctor Perry in the neck would not have been able to produce, wouldn’t have been able to produce, these contusions of the musculature of the neck.”16
Ignoring Humes’s comments above, Commissioner Allen Dulles then completely changed the subject.17
In later years, J. Thornton Boswell, the pathologist who assisted Humes, actually described seeing, on that same night, the remains of the bullet hole itself, “part of the perimeter of a bullet wound in the anterior neck”,18 and they concluded that night that the bullet exited the throat.19 When talking to the ARRB in 1996, Humes denied seeing the remains of the bullet wound, or knowing anything about its existence.20
The lead photographer, John Stringer, described the pathologists putting their fingers into the gaping hole trying to feel for anything sharp, looking for bullet fragments, in other words.21 John H. Ebersole, M.D., Acting Chief of Radiology, said that Humes had been in touch with the Parkland doctors that same night, and, clearly, had been informed of the bullet wound in the throat.22 (This is not a comprehensive treatment of the subject; there is yet other testimony relative to this issue not included here.)
Comic Relief: Humes “Explains”
“And we wondered, where’s the bullet? You know. Should have called Dallas right then and there. It would have saved me a lot of worry and grief for several hours, because x-rays hadn’t found it for us. Like it could have been in his thigh or it could have been in his buttock. It could have been any damn place …”23
So, it could have gone any damn place—except a few inches away out the hole in the front?
“We didn’t know where it went. It was obvious after we talked to the doctors the next morning where it went. It went out. That’s why we couldn’t find it. And we weren’t going to spend the rest of the night there, you know. Meantime, George Burkley is telling me, you know, the family wants to get out of here sometime tonight. Then we proceeded with the dissection of the lungs, heart and abdominal contents and so forth.”24
Note: Kennedy was not shot in the abdomen.
“… it wouldn’t make a great deal of sense to go slashing open the neck. What would we learn? Nothing you know.”25
Have sympathy for the late James Humes. He not only had to cover his own ass, he had to cover the collective ass of those who were pressuring him to come up with the “right” answers. He never did seem sure of the script.
Was it an Entrance Wound?
We have no way of knowing what the nature of Kennedy’s throat wound was but, considering all the lies told about it, Humes et al. probably thought it was an entrance. Based on the wound’s characteristics as reported, nothing seems to justify declaring it an entrance or an exit although, grossly, it was most typical of an entrance.
- Exit wounds can be small;
- Ragged wounds can be entrances;
- Entrance wounds need not have abrasion collars, but often do;
- Shored exit wounds always have pronounced abrasion collars.
- Non-shored exit wounds do not have abrasion collars.
One thing does seem certain: if the wound had been an exit, the bullet had to have exited above the shirt; it could not have gone through the shirt (the bottom part of the collar band), as alleged. This would have created a “shored wound.” In shored wounds, an obvious abrasion collar is created26 with little bits of skin hanging (like the flakes of a sunburn) as the shoring material—which usually sticks to the wound—is pulled off the victim.27
Furthermore, skin would have been left behind on the shirt: upon exiting, the bullet would have crushed the skin against the shirt on its way out, skin that would have been visible to the naked eye.28 The FBI would surely have loudly announced such evidence had they found any.
Kennedy’s throat wound did not have the wide, pronounced abrasion collar of a shored exit wound, but it apparently did have the abrasion collar of an entrance wound.29
As mentioned above, exit wounds can be small, but would a jacketed bullet travelling at medium high velocity through the loose, wrinkled, tanned, leathery skin of Kennedy’s neck leave a small wound?
Or—unhindered by any shoring material—would the bullet pull the skin forward on its way out, tenting the skin, creating the lacerations of a typical “stellate” wound of exit?
(All of the small exit wounds in the photos that I could find were in what looked like taut, young skin in areas not unexposed to the sun and not subjected to a lot of stretching, and wrinkle-causing movement, like the neck and wrists.)
For more on the subject of bullet wounds (including photographs and additional references) please see my article, “Trajectory of a Lie Part I. The Palindrome” at www.history-matters.com.
Conclusion
Commander James Humes testified that, on the night of the autopsy, the only abnormality seen in Kennedy’s throat was a tracheotomy incision. For the following reasons, this seems to have been a cover story:
- Context: there was an entrance wound, only inches away, in the back;
- The incision was larger than one for a typical tracheotomy, though, by itself, this is not reason to suspect trauma;
- The strap muscles were severed; this is not done in routine tracheotomies;
- Humes testified he saw bruising in the throat muscles that he said he knew could only have occurred during the motorcade, when the president’s heart was still functioning normally;
- Other doctors testified that they all knew of the bullet wound in the throat;
- Part of the perimeter of the hole created by the bullet was seen.
By denying awareness of the wound, Humes avoided documenting its nature. (He also avoided properly documenting the back and head wounds, all for the same reason apparently.)
A few years later, in an apparent effort to support Humes’s story, the surgeon who performed the incision, Malcolm Perry, M.D., described it as small enough to be typical. This same surgeon was most accommodating when it came to revising other trajectory-related details. Nearly 30 years later, Commander Humes himself reported the incision as small, radically contradicting his own testimony to provide a description that just happened to agree with Malcolm Perry’s.
It is also possible that each doctor simply had a malfunction of memory.
ADDENDUM
Standard Response to Penetrating Wounds of the Neck
What was the standard emergency response to a penetrating injury of the throat—whether or not the trachea (windpipe) is injured, and whether or not there is another life-threatening wound?
Exploratory surgery—however quick and limited—was and is the standard. The incision Perry made was apparently similar to the one shown in the diagram below:30
According to the 1971 issue of the American Journal of Surgery, the performance of an “exploratory” in these circumstances had been standard since World War II:
“The general surgical principle of mandatory exploration of all penetrating wounds has become established during the past three decades.” 31
Parkland Policy on Penetrating Neck Wounds
“Since 1957 it has been the policy at Parkland Memorial Hospital to explore virtually all penetrating wounds of the neck regardless of the clinical impression as to the severity of the injury …”
“The incision was planned to allow full exposure of the tract of injury. Proximal and distal control of the major vessels was also considered in the length and position of the incision. The sternocleidomastoid (“strap”) muscle and/or other neck muscles were taken off the insertion or transected whenever necessary to provide adequate exposure.”32
The textbook Principles of Trauma Care contains a chapter written by Malcolm Perry, “Penetrating Wounds of the Neck.”33 Perry’s list of findings that indicate the need for exploration include some that applied to Kennedy:
- Bleeding
- Large hematoma
- Shock
- Respiratory distress
- Subcutaneous emphysema
- Blood in the oropharynx
Finally, an exploratory is even appropriate in the absence of these signs because life-threatening damage can hide behind a superficial looking wound. The authors of the 1971 paper discovered the following:
“… one third of the patients with injury to a major structure had no clinical evidence for this. This latter group included one patient with a through and through bullet wound of the carotid artery.”34
Notes
1 D. L. Breo, “JFK’s death-the plain truth from the MD’s who did the autopsy.” Journal of the American Medical Association 1992; 267: 2794-2803, here p. 2798.
2 Autopsy Report. MD3, ARRB Master Set of Exhibits.
3 J. J. Humes, Warren Commission Hearings, Vol. II, p. 361 (“some 7 or 8 cm in length”).
4 D. S. Lifton, Best Evidence. Carroll & Graff, 1980, p. 238.
5 Autopsy Report.
6 WCH II, p. 361.
7 Lifton, p. 238.
8 Breo, p. 2798.
9 M. Perry, Warren Commission Hearings, Vol. VI, p. 10.
10 WCH VI, p. 10.
11 Perry, Warren Commission Hearings, Vol. III, p. 370.
12 Perry, ARRB Testimony, August 17, 1998, pp. 24-25.
13 Humes, HSCA Testimony, September 7, 1978, p. 330.
14 WCH II, p. 367.
15 WCH II, p. 367.
16 WCH II, p. 368.
17 WCH II, p. 368.
18 J. T. Boswell, HSCA Testimony, August 7, 1977, pp. 8, 12.
19 Boswell, ARRB Testimony, February 26, 1996, pp. 34, 45.
20 Humes, ARRB Testimony, February 13, 1996, p. 115.
21 J. Stringer, ARRB Testimony, July16, 1996, pp. 191-2.
22 J. H. Ebersole, HSCA Testimony, 1978, p. 20; pp. 51-52.
23 Humes, ARRB Testimony, p. 113.
24 Humes, ARRB Testimony, p. 113.
25 Humes, ARRB Testimony, p. 36.
26 V. J. M. Di Maio, Gunshot Wounds, Practical Aspects of Firearms, Ballistics, and Forensic Techniques, Second Edition. CRC Press, 1999.
27 J. C. Aguilar, “Shored gunshot wounds of exit.” American Journal of Forensic Medicine and Pathology 1983; 4(3): 199-204.
28 Aguilar, “Shored gunshot wounds of exit.”
29 M. Perry, HSCA p. 302; C. Baxter, Warren Commission Hearings, Vol. VI, p. 42.
30 For the diagram: J. D. Saletta, R. J. Lowe, L. T. Lim, J. Thornton, S. Delk, and G. S. Moss, “Penetrating trauma of the neck.” Journal of Trauma and Acute Care Surgery 1976; 16(7): 579-587; D. C. Blass, E. C. James, R. J. Reed, C. W. Fedde, and A. L. Watne, “Penetrating wounds of the neck and upper thorax.” Journal of Trauma and Acute Care Surgery 1978; 18(1): 2-7.
31 “Exploratory since WW II”: C. Ashworth, L. F. Williams, and J. J. Byrne, “Penetrating wounds of the neck. Re-emphasis of the need for prompt exploration.” American Journal of Surgery 1971; 121: 387-391.
32 Parkland: R. F. Jones, J. C. Terrell, and K. E. Salyer, “Penetrating wounds of the neck: an analysis of 274 cases.” Journal of Trauma and Acute Care Surgery 1967; 7(2): 228-237.
33 M. Perry, Chapter 16, “Penetrating Wounds of the Neck.” In: G. T. Shires, ed., Principles of Trauma Care, Third Edition. McGraw-Hill Book Company, 1985.
34 Ashworth, Williams, Byrne, “Penetrating wounds of the neck.”